Cosmetic Dentist NYC — Smile Design, Veneers & More
Cosmetic dentistry done well is a planned sequence — whitening, gum contour, then restoration — not a menu of unrelated procedures.
Cosmetic dentistry in NYC at Centre Dental, planned as a sequence rather than a menu. From a single bonded edge to a complete smile design, the treatment order is mapped — and explained — before any enamel is touched.
- 95.5%
- porcelain veneer survival at 10 years
- 96.81%
- lithium disilicate veneer survival (~10 yrs)
- 4.9 ★
- 226 Google reviews
The concerns patients bring to a cosmetic consultation
Patients do not arrive asking about lithium disilicate or bonding substrates. They arrive with a specific, persistent concern: a chipped incisal edge, a single discolored tooth, a shade that no longer matches, or apprehension about the over-treated look they have seen elsewhere. A sound cosmetic result depends less on any single procedure than on the order in which procedures are performed — which is why the consultation exists.
A specific, persistent flaw
A chip, a diastema, a darkened tooth, or a drifted shade — cosmetically minor, but visible in every photograph and video call.
Concern about over-treatment
The most common fear we hear is of the uniform, opaque, obviously restored look. Conservative planning — treating only what needs treating — is the safeguard.
Uncertainty about where to start
Whitening, bonding, veneers, and gum contouring interact. Performed in the wrong order, results are compromised; sequenced correctly, each step protects the next.

A plan that fixes what bothers you — in the order that makes it last.
Cosmetic dentistry is the branch of dentistry focused on the appearance of your teeth and gums: whitening, composite bonding, porcelain veneers, gum reshaping, and full smile makeovers. The result you want isn't one procedure — it's the right combination, sequenced correctly. Whitening before veneers so the shade matches. Gum contouring before crowns so the tissue is stable. Health confirmed before aesthetics so the work doesn't fail early. Done in the right order, the outcome reads as an improved version of you — not obviously dental work.
Book a smile-design consultationUnderstand it fully
The clinical picture — from consultation to a smile that holds up
At a glance
- 95.5%1
- porcelain veneer survival at 10 years
- 96.81%2
- lithium disilicate veneer survival (~10 yrs)
- ~43%3
- report temporary sensitivity after whitening
Cosmetic dentistry is a sequence, not a menu
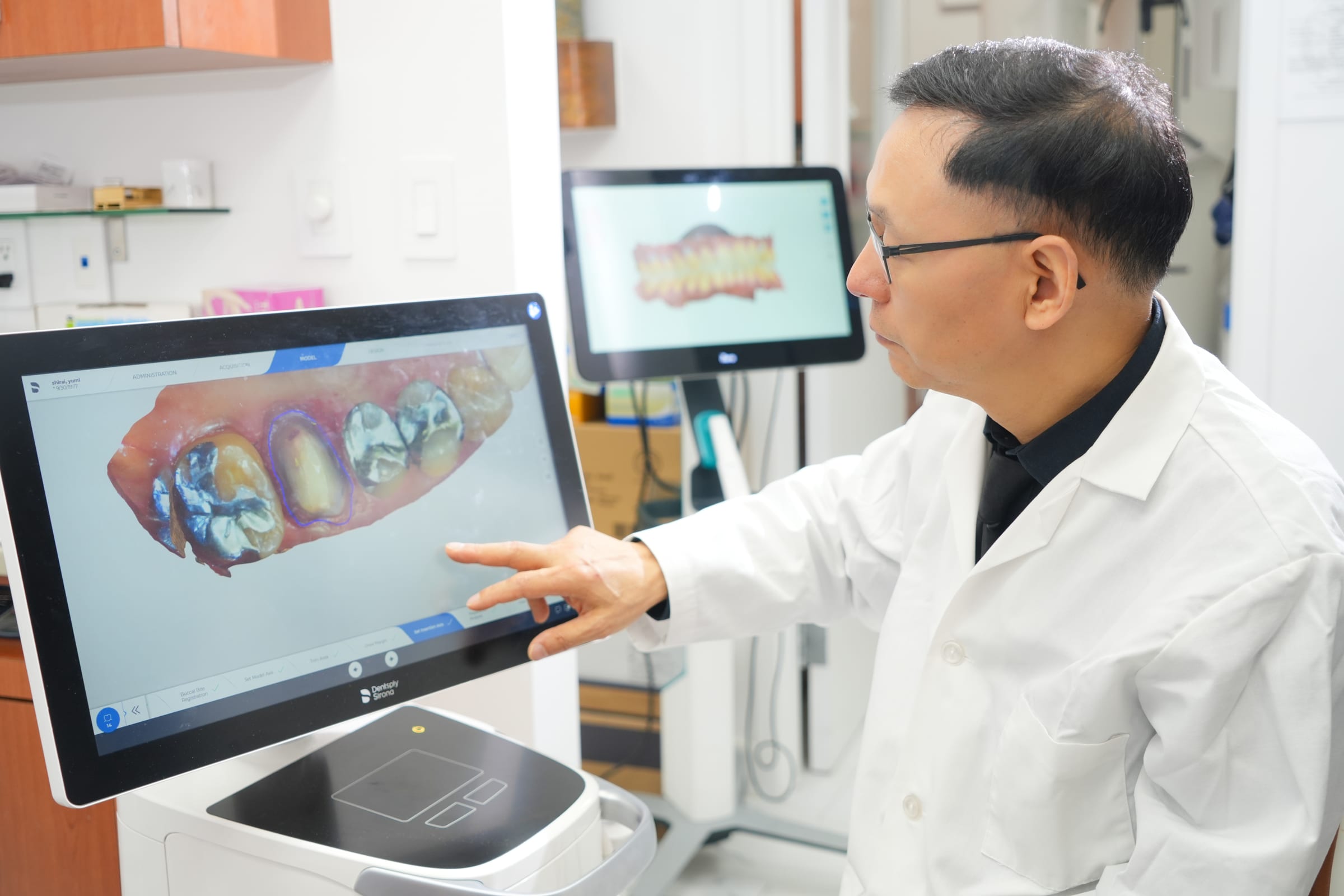
The single most common mistake we see comes from social-media research: choosing a procedure before understanding the starting point. Cosmetic dentistry is not an à la carte list — it's a sequence, where each step depends on the one before it. The consultation exists to map that order. We photograph your teeth under standardized lighting, take digital X-rays, and document how your teeth meet (your occlusion) before discussing anything aesthetic. Order matters clinically: whitening must finish before veneers are fabricated, because the ceramic shade is matched to your final tooth color — whiten afterward and the natural teeth lighten while the veneers stay put, creating a mismatch. Gum contouring should precede crowns so the tissue architecture is stable before the final restoration is placed. And function comes first — cavities restored, gum health confirmed — because cosmetic work placed over an unhealthy foundation fails prematurely. This is the Centre Method: plan the whole arc, then execute it in the order that protects the result.
The building blocks — bonding, veneers, whitening, and gum reshaping
A smile design draws on a small set of well-understood tools. Composite bonding applies a tooth-colored resin directly to the tooth in a single visit — no enamel removal, repairable, and reversible — which makes it the least invasive way to close a small gap or rebuild a chipped edge. Porcelain veneers are thin, laboratory-fabricated ceramic shells (roughly 0.3–0.7 mm) bonded to the front of a tooth to change color, shape, and length permanently. Professional whitening oxidizes pigment inside the enamel to lighten the tooth itself rather than coat it. Gum reshaping — often done with our Solea laser — corrects a gummy smile or uneven tissue heights so the teeth frame correctly. Where teeth are crowded or spaced, Invisalign can align them first, so the cosmetic work sits on a corrected foundation instead of masking the problem. Which tools you need, and in what order, is exactly what the consultation decides.
0.3–0.7 mm
Reversible first — why we ask about bonding before veneers
There is a one-way door in cosmetic dentistry, and it's worth naming clearly: conventional veneer preparation removes 0.3–0.7 mm of enamel, and enamel does not grow back. Once it's removed, that tooth is committed to some form of artificial covering for the rest of your life, through several replacement cycles over decades. That is not an argument against veneers — for many patients they are precisely the right choice. It's the reason we ask, every time, whether composite bonding can accomplish what you actually want first. Bonding requires no enamel removal and can be adjusted or reversed, so when it will achieve the goal, it should be the first conversation, not the second thought. If your concern genuinely needs the permanence, translucency, and stain resistance of ceramic, veneers are the answer — but you'll make that decision knowing the trade-off, not discovering it later.
The materials — why modern ceramics look and last the way they do
The aesthetics of a restoration are largely a materials story. Older feldspathic porcelains were beautiful but comparatively fragile; the shift to lithium disilicate — a glass-ceramic (marketed as IPS e.max) — brought a step-change in durability without sacrificing the way the material transmits and scatters light like natural enamel. According to PubMed, a 2024 systematic review and meta-analysis of ceramic laminate veneers found lithium disilicate reached a pooled survival of 96.81% at roughly 10 years, with markedly lower technical, aesthetic, and biological complication rates than feldspathic or leucite-reinforced ceramics (Klein et al., J Esthet Restor Dent 2024, DOI). Zirconia (zirconium dioxide) offers even higher strength and is used where forces are heavier, though long-term veneer data for it remains thinner. The practical takeaway: material selection is a clinical decision matched to the tooth, the bite, and the aesthetic demand — not a luxury upgrade. The right ceramic in the right place is what makes a veneer difficult to distinguish from the tooth beside it.
Your next step
Wondering if cosmetic dentistry is right for you?
A free consultation includes an exam and a written plan — no pressure, no upsell.
Bonding substrate — the quiet detail that decides longevity
How long a veneer lasts depends heavily on what it's bonded to. Adhesion to enamel is stronger and more durable than adhesion to the dentin underneath it — which means over-aggressive preparation that cuts through enamel into dentin is a technical error, not a stylistic one. According to PubMed, a clinical study of porcelain laminate veneers found significantly higher failure rates when preparations exposed severe dentin versus staying in enamel or minimal dentin exposure (Öztürk & Bolay, J Adhes Dent 2014, DOI), and a controlled laboratory fatigue study confirmed enamel-bonded lithium disilicate veneers withstood significantly higher loads than dentin-bonded ones (Gierthmuehlen et al., J Esthet Restor Dent 2022, DOI). This is why a conservative, enamel-preserving preparation is one of the most consequential decisions in the whole procedure — and why we plan preparation depth deliberately rather than removing more tooth than the result requires.
Cosmetic vs. restorative — the insurance line no one explains
Whether a procedure is classified as cosmetic or restorative changes what your insurance may cover — and most offices never explain the difference. A veneer placed purely to improve the color of a healthy tooth is aesthetic and typically isn't covered. The same veneer placed over a tooth with documented structural damage — decay, fracture, significant wear — may qualify for partial restorative coverage. The distinction is clinical and it's documentable. We record the rationale for each treatment and submit for any applicable coverage before you commit, so you know what your plan will and won't contribute. For anything that remains out of pocket, financing options let the cost be phased over time rather than paid all at once. You'll see the full, itemized picture in writing at your consultation — never a surprise at checkout.
Combining treatments — what good sequencing produces
A full smile transformation is several procedures in a planned order. A representative case: whitening establishes the target shade, upper veneers are fabricated to match it, gum contouring balances the tissue proportions, and bonding refines the secondary teeth that fall outside the veneer scope. Each step relies on the one before it, and the sequencing decisions made at consultation are what determine whether the final result looks coordinated or mismatched. We use a digital smile preview to show proportions and shade before any preparation begins — not as a guarantee, but as a shared reference for the conversation about what you want. The written plan lists each procedure, its timing, and its cost separately. Patients who understand what each phase accomplishes, and why it comes when it does, consistently report higher satisfaction — because their expectations were built on clinical reality rather than a filtered photo. It's the same principle we bring to more complex work, from Invisalign alignment to dental implants when a tooth is missing entirely.
Protecting the result — night guards, habits, and maintenance
The most avoidable way to lose good cosmetic work is grinding. Ceramic is fracture-resistant under normal chewing, but bruxism generates forces far outside that range, and a single episode can catastrophically fracture a veneer that would otherwise last well over a decade. If you clench or grind, a custom night guard is not optional — it distributes force across all your teeth instead of concentrating it at veneer margins. Beyond that, maintenance is straightforward and familiar: twice-daily brushing with a soft-bristle toothbrush, non-abrasive fluoride toothpaste, daily flossing, and professional cleanings roughly every six months. The bonding margin at the gumline can pick up stain from coffee, tea, and red wine over time — that's polished at routine visits. Avoid biting fingernails, opening packaging with your teeth, or biting directly into very hard foods. The restorations do the aesthetics; these habits do the longevity.
Related at Centre Dental
What patients say
Reviewed, on Google
I came for an emergency root canal treatment and I did not regret choosing this place. It was quick and painless. Plus, everyone was very quite friendly.
I recently had a dental cleaning at Centre Dental, and I had a wonderful experience. The staff was friendly, professional, and welcoming. The cleaning was very thorough yet gentle, and everything was explained clearly th…
A skillful Dentist who goes the Extra Miles I have been flying to NYC from Florida multiple times to this dental office. Dr. Shi has been working on my upper full mouth teeth transplant for over half a year. So far I ha…
Concerned about comfort, bone, or cost?
These are the questions a consultation answers directly. Dr. Shi reviews your 3D CBCT scan, evaluates your bone and candidacy, and outlines your options, treatment timeline, and estimated cost — including what your insurance may cover.
Thinking about it
The questions we hear first
What does cosmetic dentistry actually include?
Cosmetic dentistry covers procedures that improve the appearance of your teeth and gums — teeth whitening, composite bonding, porcelain veneers, gum reshaping, and full-mouth smile makeovers. Many also carry a functional benefit: a veneer can restore a structurally damaged tooth, and bonding repairs a chipped edge. The line between cosmetic and restorative matters for insurance — a veneer on a damaged tooth may receive partial coverage, while the same veneer on a healthy tooth for purely aesthetic reasons typically does not. We document the clinical rationale and check your coverage before any procedure begins.
Should I get veneers or bonding?
It depends on what you're correcting and how permanent you want the change to be. Composite bonding applies tooth-colored resin directly to the tooth in one visit, with no enamel removal — it's adjustable and reversible, which makes it the right first option for small chips, minor gaps, and edge repairs. Porcelain veneers are laboratory-made ceramic shells bonded permanently to the tooth; they deliver the most durable color and shape change and resist staining, but preparing for them removes enamel, which does not grow back. Because that step is irreversible, we evaluate every patient for bonding suitability first — if bonding can accomplish the goal, that's the conversation we have before recommending veneers.
Will cosmetic work look natural, or will people be able to tell?
Done well, it reads as an improved version of you rather than obvious dental work. Modern ceramics — lithium disilicate and translucent zirconia — transmit and reflect light much like natural enamel, so properly placed restorations are difficult to distinguish from real teeth. According to PubMed, a 2024 meta-analysis found lithium disilicate veneers combine that lifelike optical behavior with high long-term survival (Klein et al., J Esthet Restor Dent 2024, DOI). We check shade under multiple lighting conditions and use a digital smile preview to evaluate proportions before any fabrication — the goal is consistency with your face and neighboring teeth, not a uniform white slab.
Why does the order of treatment matter so much?
Sequence errors are one of the most common sources of cosmetic disappointment. Whitening after veneers are already placed lightens your natural teeth while the veneers stay the same shade — an instant mismatch. Gum contouring after crowns can expose crown margins as the tissue heals. Bonding done before orthodontic alignment often has to be removed and redone. The consultation is where these decisions get made and documented. We map the planned order and explain why each step comes when it does, so you understand the rationale rather than just the schedule.
How long do cosmetic dental results last?
It varies by procedure and by material. According to PubMed, a 2021 systematic review of porcelain laminate veneers reported a 10-year cumulative survival of 95.5% (Alenezi et al., J Clin Med 2021, DOI), and a 2024 meta-analysis put lithium disilicate veneers at 96.81% at roughly 10 years (Klein et al., DOI). Composite bonding lasts a shorter span and is refreshed or repaired more often; whitening fades over time and is maintained with periodic touch-ups; gum contouring results are generally permanent. The biggest variable after material choice is behavior — unprotected grinding, biting hard objects, and heavy dark-beverage habits all shorten restoration life. We cover realistic maintenance expectations at your consultation.
Are cosmetic procedures painful?
Most involve little discomfort. Composite bonding and laser gum contouring are generally well tolerated with minimal or no anesthesia. Veneer preparation is done under local anesthesia, and mild post-procedure sensitivity around the prepared teeth is common, usually resolving once the final restorations are bonded. Whitening causes temporary sensitivity in a meaningful share of patients — according to PubMed, a randomized clinical trial found roughly 43% of participants reported some sensitivity during bleaching, rising to about 71% with higher-concentration gels, and it typically settles within a day or two (Basting et al., Oper Dent 2012, DOI). We document your sensitivity history at the consultation and adjust protocols accordingly. If you're anxious about any of it, ask about our dental-anxiety support options.
Does insurance cover cosmetic dental work, and can I finance it?
Most purely cosmetic procedures aren't covered because they're classified as elective. But the cosmetic-versus-restorative line isn't always clear-cut: a veneer or crown placed over a tooth with documented decay, fracture, or significant wear may qualify for partial restorative coverage, while the same restoration on a healthy tooth for aesthetics alone typically won't. We identify which of your procedures have a legitimate restorative rationale, document it properly, and submit for any coverage you may be entitled to before treatment starts. For out-of-pocket costs, financing options are available and treatment can be phased across appointments. You'll review the itemized plan and your insurance picture together at the consultation.
How long does a full smile makeover take from start to finish?
Single procedures are fast: whitening and bonding can often be completed in one appointment. Conventional porcelain veneers usually take two visits over two to three weeks — or a single visit with CEREC same-day milling. A full-mouth transformation typically spans several months, especially when preparatory work — gum treatment, Invisalign alignment, or implant placement — has to be completed before the cosmetic restorations go on. We provide a written timeline at your consultation with each phase dated, so you can plan around work and personal commitments.
The path
Your journey, start to finish
Smile-design consultation & records
We photograph your teeth under standardized lighting, take digital X-rays, and document your bite before discussing aesthetics. You'll leave understanding your starting point — and which concerns are cosmetic, which are functional, and which need treating first.
Your sequenced plan (and a digital preview)
A written treatment plan lays out each procedure, its order, its timing, and its cost separately. We use a digital smile preview to show proportions and shade, and review your insurance and financing options — so you decide what to do now and what to phase over time.
Foundation first, then aesthetics
Health comes before beauty: cavities restored, gum tissue confirmed healthy, alignment corrected with Invisalign if needed, and whitening completed before any ceramic is fabricated — so the final shade matches and the work sits on a stable base.
Restoration & long-term maintenance
Bonding, veneers, crowns, or gum reshaping are placed in the planned order by Dr. Shi. We finish with a maintenance plan — a night guard if you grind, touch-up whitening trays, and regular cleanings — so the result you chose is the result you keep.
Explore Further
Related Services
Porcelain Veneers
Thin ceramic shells that permanently correct chips, gaps, and discoloration with minimal, enamel-preserving preparation.
Learn moreTeeth Whitening (Zoom)
Professional in-office Zoom whitening and custom take-home trays — the shade foundation for any smile design.
Learn moreInvisalign Clear Aligners
Removable clear aligners that straighten teeth first, so cosmetic work sits on a corrected foundation.
Learn moreSame-Day Crowns (CEREC)
CEREC-milled ceramic crowns and veneers designed and placed in a single visit — no temporary phase.
Learn moreCosmetic Dentistry Near You in NYC
Start here
Schedule your consultation
In a single visit, Dr. Shi reviews your 3D scan, assesses your candidacy for cosmetic dentistry, and provides a written treatment plan with cost and insurance details — so you can decide with all the facts.
Extensive full-arch reconstruction experience by Dr. Shi
3D-guided precision, placed by an experienced surgeon
Bilingual — English, Mandarin, Cantonese
Live clinic hours · 139 Centre St, Lower Manhattan, NYC