Pinhole Gum Rejuvenation NYC — No Scalpels, Same-Day Results
Recession coverage through a single needle-sized entry point — no scalpel, no sutures, no palatal donor site.
The Pinhole Surgical Technique in NYC, performed by Dr. John Shi. In suitable cases, receded gum tissue is repositioned over the exposed roots through one needle-sized opening — no donor wound, with visible improvement the same day.

- 81.2%
- complete root coverage, Miller Class I/II (originating PST study)
- 94.0%
- mean recession-defect reduction, Class I/II
- 4.9 ★
- 226 Google reviews
Why gum recession warrants treatment
Patients seldom present asking about Miller classifications or gingival biotype. They present because their teeth appear longer, because exposed roots have become sensitive to cold, or because a prior mention of palatal grafting has kept them from proceeding. Recession is progressive: exposed root surfaces lack enamel and are more vulnerable to abrasion, sensitivity, and root-surface decay. The sections below explain the technique, the evidence behind it, and — candidly — the cases it is not suited for.
Visibly lengthening teeth
A receding gumline progressively exposes the darker root surface — an aesthetic change, and an early marker of tissue loss that tends to advance if unaddressed.
Root-surface sensitivity
Exposed roots have no enamel layer. Cold, sweet stimuli, and even routine brushing can produce sharp, localized sensitivity.
Apprehension about traditional grafting
Conventional gum grafting harvests donor tissue from the palate, creating a second surgical site. For many patients that recovery — not the recession — is what delays treatment.

Your own gum tissue, moved back where it belongs — through a single tiny opening.
The Pinhole Surgical Technique treats receding gums by loosening your existing gum tissue and gently sliding it back down over the exposed roots, all through one needle-sized entry point. Because it repositions the tissue you already have, there's no scalpel incision, no sutures, and — critically — no donor site on the roof of your mouth. Collagen strips slipped through the same opening hold the tissue in its new position while it reattaches. Covering the root again protects it from decay and sensitivity, restores a natural-looking gumline, and for a suitable candidate, does it in a single visit.
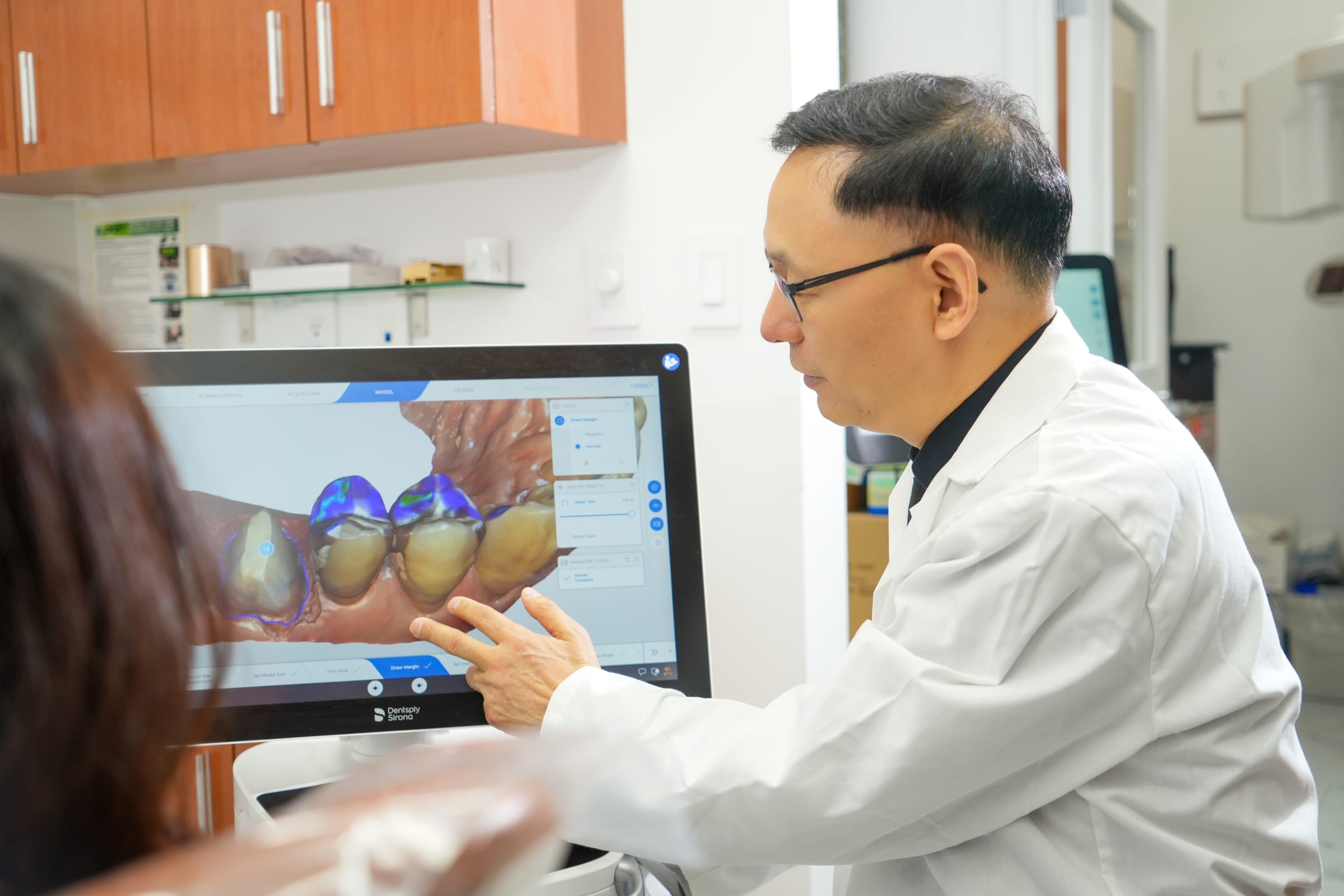
Schedule a gum recession consultationFrom our operatory
See the treatment, not just the words
The regenerative side of gum treatment — how supporting tissue is rebuilt and stabilized around the teeth.
Understand it fully
The clinical picture — from gumline to lasting coverage
At a glance
- 81.2%1
- complete root coverage, Miller Class I/II (originating PST study)
- 94.0%1
- mean recession-defect reduction, Class I/II
- 63.6% vs 65.4%2
- PST vs connective-tissue graft root coverage at 1 yr (not significant, P=.72)
- 22.5%3
- of US adults 30+ have ≥3 mm gum recession on ≥1 tooth

What the Pinhole Surgical Technique actually is
The Pinhole Surgical Technique (PST) is a minimally invasive, scalpel-free approach to gingival recession developed by periodontist Dr. John Chao. Instead of harvesting a connective tissue graft from the palate, PST uses a single needle-sized entry point to release the gingiva and glide it coronally — toward the crown of the tooth — over the exposed root surface. Small strips of resorbable collagen are placed through that same opening to stabilize the repositioned tissue and act as a scaffold for reattachment. There are no releasing incisions, no sharp dissection, and no sutures when a bioresorbable membrane is used. According to PubMed, the originating study of PST reported a mean procedure time of roughly 22 minutes across treated sites, with minimal postoperative complications (Chao, Int J Periodontics Restorative Dent 2012). It's a technique with a specific, evidence-backed lane — and part of doing it responsibly is being clear about where that lane ends.
Are you a candidate? What actually determines suitability
The single most important factor is your recession classification. PST is validated for Miller Class I and II recession. Class I is recession that has not reached the mucogingival junction, with no loss of bone or tissue between the teeth. Class II reaches or extends past the mucogingival junction but still has no interproximal bone loss — full root coverage remains achievable in both. Miller Class III and IV involve interproximal bone or soft-tissue loss, and PST is not appropriate for them; those cases are better served by conventional grafting or other periodontal surgery. A thin gingival biotype — less than roughly two to three millimeters of attached tissue — is also a disqualifier, because there simply isn't enough tissue to reposition reliably. Some patients are surprised to be told they don't qualify after expecting to be a candidate, which is exactly why an honest clinical evaluation with periodontal probing comes before any promise of treatment.

How PST compares to a connective tissue graft — an honest comparison
The connective tissue graft (CTG), usually combined with a coronally advanced flap, remains the most established root-coverage procedure, with the deepest body of long-term evidence across the widest range of recession presentations. Its trade-off is the palatal donor site — a second surgical wound that is the primary source of postoperative discomfort in conventional grafting. PST's central advantage is that it eliminates that donor wound entirely. Importantly, the two are clinically comparable in coverage for the cases PST is designed for. According to PubMed, a split-mouth randomized trial co-authored by Dr. Chao found no significant difference in one-year outcomes between PST with a collagen membrane and CAF with a connective tissue graft — mean root coverage of 63.6% versus 65.4% (P = .72), and near-identical recession reduction of about 1.97 mm each (Shibly et al., Compend Contin Educ Dent 2025). The takeaway isn't that one technique wins; it's that for a well-selected Class I or II patient, PST can deliver graft-comparable coverage without the second wound.
Your next step
Wondering if pinhole gum rejuvenation is right for you?
A free consultation includes an exam and a written plan — no pressure, no upsell.
The materials — collagen, membranes, and why they matter
Collagen is the structural protein that makes up much of your own gum's connective tissue, which is why a resorbable collagen membrane is a natural fit as the internal scaffold in PST. Slipped through the pinhole opening, the collagen strips brace the repositioned gingiva against the tooth and guide new tissue attachment before the body gradually breaks the material down and replaces it with your own tissue. Some clinicians reinforce or accelerate the response with adjuncts studied in the literature — platelet-rich fibrin (PRF), a concentrate drawn from a patient's own blood, is one that has been evaluated alongside PST. The right material choice is matched to your anatomy and recession pattern at the planning stage, not applied as a one-size-fits-all default.
22.5%
Why gums recede in the first place — and why that governs the outcome
Gingival recession is common and multifactorial. According to PubMed, national survey data estimate that roughly 22.5% of U.S. adults aged 30 and older have at least one tooth surface with 3 mm or more of recession, with prevalence and severity rising steadily with age (Albandar & Kingman, J Periodontol 1999, NHANES III). The usual drivers are aggressive or abrasive toothbrushing, periodontal (gum) disease, tooth position, clenching and grinding forces, and sometimes orthodontic movement. This matters for PST because covering the root treats the visible result, not the cause. If the underlying behaviour or condition continues — a hard-bristled scrubbing technique, untreated gum disease, or unmanaged grinding that may call for a night guard — recession can recur regardless of how well the tissue was repositioned. Durable coverage is a partnership between the procedure and what changes afterward.
Recovery and what the first weeks feel like
Because PST avoids a palatal donor wound, recovery is generally more comfortable than conventional grafting for most patients. The procedure itself is done under local anaesthesia, so you feel pressure rather than pain. Afterward, expect mild soreness, tenderness, and some swelling that is usually most noticeable in the first two to three days and manageable with over-the-counter analgesics for the large majority of patients. A soft-food diet protects the repositioned tissue for the first week or two while it integrates, and vigorous rinsing and strenuous activity are best avoided for the first few days. A short follow-up visit confirms the tissue has held its new position and is attaching as planned. Most people are back to their normal routine quickly — the absence of that second wound is the difference nearly every patient notices.
Long-term results, maintenance, and where PST fits in your care
When patients are properly selected, the coverage PST achieves is meant to last — but longevity is earned through maintenance, not assumed. The most reliable predictor of sustained coverage is addressing the original cause and keeping up with periodontal maintenance: correcting brushing technique, controlling gum inflammation, and managing grinding forces. Patients who skip maintenance cleanings are the group most likely to see coverage regress over time. Recession is also frequently one finding within a broader preventive care picture, so at Centre Dental it's evaluated in that context — alongside your gum health, bite, and habits — rather than treated as an isolated cosmetic fix. For the candidate who fits the Miller Class I or II profile with adequate tissue, PST is a genuinely elegant option; for everyone else, we'll tell you plainly and point you to the approach your anatomy actually calls for.
Related at Centre Dental
What patients say
Reviewed, on Google
I came for an emergency root canal treatment and I did not regret choosing this place. It was quick and painless. Plus, everyone was very quite friendly.
I recently had a dental cleaning at Centre Dental, and I had a wonderful experience. The staff was friendly, professional, and welcoming. The cleaning was very thorough yet gentle, and everything was explained clearly th…
A skillful Dentist who goes the Extra Miles I have been flying to NYC from Florida multiple times to this dental office. Dr. Shi has been working on my upper full mouth teeth transplant for over half a year. So far I ha…
Concerned about comfort, bone, or cost?
These are the questions a consultation answers directly. Dr. Shi reviews your 3D CBCT scan, evaluates your bone and candidacy, and outlines your options, treatment timeline, and estimated cost — including what your insurance may cover.
Thinking about it
The questions we hear first
Am I a candidate for Pinhole gum rejuvenation?
PST is validated for Miller Class I and II recession. Class I is recession that does not reach the mucogingival junction with no bone loss — 100% root coverage is achievable. Class II reaches or extends past the mucogingival junction, still with no interproximal bone loss, and full coverage remains possible. Miller Class III and IV involve interproximal bone loss and are not appropriate for PST — those need conventional grafting or other approaches. A thin gingival biotype (less than roughly two to three millimeters of attached tissue) is a disqualifier many patients don't expect. A clinical evaluation with periodontal probing measurements determines your classification before any treatment is recommended.
How does Pinhole compare to a traditional connective tissue graft?
Both aim to cover exposed root surfaces, and for the cases PST is designed for, the coverage is comparable. A split-mouth randomized trial co-authored by the technique's developer found no significant one-year difference between PST with a collagen membrane and a coronally advanced flap with connective tissue graft — around 63.6% versus 65.4% root coverage, with near-identical recession reduction. The key practical difference is that conventional grafting requires harvesting tissue from your palate, and that donor wound is the main source of postoperative discomfort. PST eliminates that second surgical site. Conventional grafting still has the deeper long-term evidence base and works across a wider range of recession, including Class III and IV, so neither is universally superior — the right choice follows your classification and anatomy.
Is Pinhole just marketing hype?
It's a fair question. PST has legitimate peer-reviewed support: the originating study reported strong root coverage in Miller Class I and II cases, and a more recent randomized trial found it comparable to a connective tissue graft at one year. The concern worth naming is that it's sometimes marketed as suitable for all recession, which it is not — it's specifically for Class I and II with adequate tissue. At Centre Dental, PST is offered only to patients who meet those criteria. Where you don't fit them, we say so and recommend the approach that does, rather than stretching one technique to cover every case.
Is the procedure painful?
Local anaesthesia is administered first, so you don't feel pain during treatment — mostly gentle pressure and movement. Afterward, expect mild to moderate soreness and some swelling in the treated area, usually most noticeable in the first two to three days and manageable with over-the-counter pain relievers for most patients. Because there's no palatal donor wound, recovery is typically more comfortable than with a conventional graft — that second wound site is the primary driver of post-op pain in traditional grafting, and PST doesn't create one.
What does Pinhole gum treatment cost in NYC?
Cost depends on how many teeth are treated and the extent of the recession, so we're transparent about it in person rather than online. At your consultation you'll leave with a written estimate for your specific case. Gum recession treatment can often be billed under periodontal procedure codes when the recession is causing documented sensitivity, root exposure, or a functional concern, and our team verifies your insurance benefits and submits supporting documentation. For any remaining balance, financing options are available so it can be spread over time.
How long do the results last?
For appropriately selected patients, the coverage is intended to last — but durability depends on addressing what caused the recession in the first place. Brushing technique, bite forces, gum health, and keeping up with periodontal maintenance appointments all determine whether the coverage holds. Patients who attend regular maintenance cleanings and correct contributing habits sustain their results most reliably; recession can recur when the underlying causes persist. We'll map out the specific maintenance plan for your case so the result you get is the result you keep.
Who is NOT a good candidate for Pinhole?
Patients who generally aren't candidates include those with Miller Class III or IV recession (which involves interproximal bone loss), a thin gingival biotype with insufficient attached tissue to reposition, active uncontrolled gum disease, or systemic conditions that impair healing. These patients are better served by a conventional connective tissue graft or another periodontal approach. Being clear about these boundaries is what separates appropriate patient selection from overpromising — and it's why the evaluation comes before any treatment recommendation.
Will treating my gums fix the sensitivity in those teeth?
Often, yes. Exposed root surfaces have no protective enamel, which is why receding gums so commonly cause sensitivity to cold, sweet, and touch. Repositioning healthy gum tissue back over the root physically covers that vulnerable surface, and many patients notice reduced sensitivity as a result. If sensitivity is your main concern, mention it at your consultation — it's part of what we assess when determining whether covering the root is the right solution or whether another issue, such as tooth decay, also needs attention.
The path
Your journey, start to finish
Consultation + periodontal evaluation
Dr. Shi examines your gumline, takes periodontal probing measurements and photographs, and determines your Miller Classification. This is where candidacy is decided honestly — you'll be told plainly whether PST fits your case, along with a clear cost and insurance estimate.
Your treatment plan (and the honest alternative, if needed)
If you're a Class I or II candidate with adequate tissue, we plan the pinhole approach. If your recession is Class III/IV or your biotype is too thin, we recommend the connective tissue graft or periodontal approach your anatomy actually calls for — never PST stretched to fit a case it wasn't designed for.
The pinhole procedure
Under local anaesthesia, a single needle-sized entry point is made. Your existing gum tissue is gently released and repositioned over the exposed roots, and resorbable collagen strips are placed through the same opening to stabilize it. No scalpel, no sutures, no palatal donor wound — often several teeth in one visit, performed by Dr. Shi himself.
Healing and long-term maintenance
Mild soreness settles within days and the collagen resorbs over the following months as the tissue reattaches. A follow-up visit confirms the result, and we build the maintenance plan — brushing technique, gum health, bite management — that keeps your coverage lasting.
Soft-tissue regeneration for receded gums
For patients whose gum disease has progressed to visible recession but whose bone support is still salvageable, the pinhole approach reframes traditional gum-graft surgery. Instead of harvesting palatal tissue and suturing it over the recession site, Dr. Shi releases the existing gum tissue through a small entry point and repositions it coronally, securing the new position with collagen strips placed through the same pinhole.
Recovery is typically shorter than traditional connective-tissue grafting because there is no donor site on the palate. For deeper underlying defects, the same visit can include guided tissue regeneration with a barrier membrane and graft material — same sequencing logic Centre Dental uses for surgical periodontal cases.
Explore the Cluster
Explore the full Same-Day Crowns
Explore Further
Related Services
Gum Disease Treatment
Treating the underlying periodontal disease that often drives recession in the first place.
Learn moreSolea Laser Dentistry
CO2 all-tissue laser for many soft-tissue procedures — often with less discomfort and faster healing.
Learn morePreventive Dentistry
The cleanings, exams, and habit coaching that protect your gumline and keep results lasting.
Learn moreMeet Dr. John Shi, DDS
Columbia-trained, performing both the surgical and restorative phases of your care himself.
Learn morePinhole Gum Rejuvenation Near You in NYC
Start here
Schedule your consultation
In a single visit, Dr. Shi reviews your 3D scan, assesses your candidacy for pinhole gum rejuvenation, and provides a written treatment plan with cost and insurance details — so you can decide with all the facts.
Extensive full-arch reconstruction experience by Dr. Shi
3D-guided precision, placed by an experienced surgeon
Bilingual — English, Mandarin, Cantonese
Live clinic hours · 139 Centre St, Lower Manhattan, NYC